These posts are educational content created by the site author, Dr. Andrew Norris, for clinical providers of all levels wishing to learn more about pediatric endocrinology.
Save The Date! Dr. Kanner has announced that she will host our annual Off To College Class on July 24, 2021 at 5-7 pm, via Zoom. Students, parents, future roommates, and any others interested are welcomed to attend. If you are interested, contact us, either through the email link at Dr. Kanner’s webpage (link) or by contacting our diabetes nursing team. The event’s flyer is immediately below.
Post by Andrew Norris, MD PhD Director, Pediatric Endocrinology & Diabetes University of Iowa Stead Family Children’s Hospital
“Don’t just look at the pH when interpreting a blood gas. If you only look at the pH, you will likely underestimate or even overlook metabolic acidosis.“
Metabolic acidosis is frequently encountered in clinical medicine. It is crucial that clinicians be able to recognize metabolic acidosis, characterize the specific type of acidosis, and assess its severity. This primer is focused on metabolic acidosis, and does not delve into other acid-base disturbances (i.e. metabolic alkalosis, respiratory acidosis and respiratory alkalosis).
Outline/topics Pearls Quick cookbook Important pitfalls What is metabolic acidosis? ◦ Background – soda & vinegar ◦ Metabolic acidosis – a simple definition ◦ Metabolic acidosis – an even simpler definition ◦ Symptoms of metabolic acidosis Diagnosis of metabolic acidosis ◦ Laboratory tests related to metabolic acidosis ◦ Blood gas interpretation in metabolic acidosis Causes of metabolic acidosis ◦ Major metabolic acidosis categories ◦ Some common causes of metabolic acidosis with elevated anion gap ◦ Some common causes of metabolic acidosis with normal anion gap ◦ Mixed acid-base disorders Footnotes
Pearls
A low serum bicarbonate usually indicates metabolic acidosis. For this reason, serum bicarbonate is a effective test for metabolic acidosis under most conditions.
Don’t just look at the pH when interpreting a blood gas. Metabolic acidosis is usually accompanied by a significant degree of respiratory compensation that brings the pH back towards normal. If you only look at the pH, you will likely underestimate or even overlook metabolic acidosis.
Determine the underlying cause. Metabolic acidosis has numerous possible causes, many of which are medical emergencies requiring timely diagnosis and institution of specific therapy.
An anion gap can help determine the type of metabolic acidosis present.
Quick cookbook
Obtain laboratory test(s): blood gas and/or serum bicarbonate
Interpret test results
Serum bicarbonate: low value indicates metabolic acidosis
Blood gas: must be fully interpreted, including
pH: low value indicates acidosis; high value indicates alkalosis
calculated bicarbonate: low value indicates metabolic acidosis
base excess: negative values below the reference range indicate metabolic acidosis
Obtain anion gap if metabolic acidosis is present.
If elevated: possible etiologies include diabetic ketoacidosis, lactic acidosis, specific inborn errors of metabolism, severe renal failure, or poisoning.
If normal: possible etiologies include GI or renal bicarbonate losses, compensation for chronic respiratory alkalosis, or hyperchloremic acidosis during resolution of DKA.
Determine the underlying cause: using additional diagnostic tests and clinical reasoning
Treat underlying cause.
Important pitfalls
Failure to fully interpret a blood gas. Often, acute metabolic acidosis is accompanied by a substantial degree of respiratory compensation (i.e. Kussmaul breathing).
Failure to determine the underlying cause. It is critical to correctly diagnosis the underlying etiology that has caused the metabolic acidosis. Some of the common causes of metabolic acidosis are medical emergencies requiring urgent specific treatments.
What is metabolic acidosis?
Background – soda & vinegar
Vinegar + soda: vinegar and sodium bicarbonate were combined, along with water, dish detergent, and trypan blue. Equivalently, ketoacids react with bicarbonate in the blood stream, causing metabolic acidosis.
The body uses a bicarbonate buffering system for maintenance of acid-base status. This is a system you may have learned as a child when playing experimenting with baking soda and vinegar. The chemistry is simple, and can be written as follows:
In health, by controlling the amount of bicarbonate (HCO3–, a base) and carbon dioxide (CO2) in the blood, the body is able to maintain pH near 7.40.
The same system is at play with baking soda and vinegar. Baking soda contains HCO3–. Vinegar is an acid, and supplies H+. When the two are combined, water and carbon dioxide gas are formed. The carbon dioxide bubbles are the fun part. The more important part, at least from a physiological view, is what happens to the pH. After equilibrium is reached, if vinegar is in excess, the pH will be acidic. Conversely, if bicarbonate is in excess, then the pH will be basic.
Metabolic acidosis – a simple definition
Metabolic acidosis occurs when the amount of acid (H+) in the blood is too high or when the amount of bicarbonate (HCO3–) is too low. (b)
Metabolic acidosis – an even simpler definition
Metabolic acidosis is present when the amount of bicarbonate (HCO3–) in the blood is too low.
Notice that this definition omits the “excess acid (H+)” part of the definition. To understand why this part of the definition can be omitted, we can turn back to the vinegar / soda experiment. When vinegar (a source of H+) is added to bicarbonate, the two react to form CO2 + H2O. Bicarbonate is depleted as this reaction proceeds. The same happens in the body when excess H+ is present – bicarbonate is depleted (c) and the serum HCO3– drops (d) .
Symptoms of metabolic acidosis
Acute metabolic acidosis is often accompanied by Kussmaul respirations, as the body attempts to reduce pCO2 in order to normalize pH. This respiratory pattern becomes more pronounced as the acidosis becomes more severe. Other symptoms are less specific but can include fatigue, weakness, tachycardia, abdominal pain and vomiting, headache, and confusion. At its severe extreme, metabolic acidosis induces coma and circulatory collapse.
Diagnosis of metabolic acidosis
Laboratory tests related to metabolic acidosis
Blood gas: A blood gas is an effective test to assess for and quantify metabolic acidosis. A blood gas measurement also informs about the respiratory component of pH (i.e. carbon dioxide). A blood gas is the primary means to distinguish whether acidosis is due to primary metabolic versus respiratory versus mixed issues. Importantly, the clinician must fully interpret the blood gas, beyond simply looking at the pH, pCO2 and pO2.
Serum bicarbonate(e): Measurement of the serum bicarbonate is also an effect means to assess for and quantify metabolic acidosis. As discussed above, a low bicarbonate indicates the presence of metabolic acidosis. There are a few circumstances when a serum bicarbonate lower than the reference range can be normal for a person, namely to compensate for respiratory alkalosis; this is detailed below.
Anion gap: Can help determine the nature of metabolic acidosis.
Chloride: Can help determine the nature of metabolic acidosis.
Units: A brief note about scientific units. In most U.S. hospitals, bicarbonate, anion gap, and chloride are all reported in mmol/L. Likewise, some of the major acidosis inducing anions, lactate and beta-hydroxybutyrate are typically reported in mmol/L. This makes internal comparison of these values simple. For example, 10 mmol/L beta-hydroxybutyrate in the serum would be expected to add 10 mmol/L to the anion gap and also to lower the serum bicarbonate by roughly the same amount.
Blood gas interpretation in metabolic acidosis
When checking for metabolic acidosis using a blood gas, it is critical to look at more than the pH. Looking at only the pH can cause one to underestimate the severity of the metabolic acidosis or even miss the presence of metabolic acidosis altogether.
To assess for metabolic acidosis, examine the following two parameters
HCO3– : calculated bicarbonate. If this is abnormally low, then metabolic acidosis is present.
“Base excess“: This is normally near zero. If it is abnormally below zero, then metabolic acidosis is present.
Complete interpretation of blood gas is beyond the scope of this primer. See footnote (f) for some free resources to learn more.
Causes of metabolic acidosis
Major metabolic acidosis categories
Elevated anion gap: A very important discriminant of the nature of metabolic acidosis is the presence or absence of an anion gap. When the anion gap is elevated, this indicates the presence of an acid. To use our vinegar–soda analogy, adding vinegar to blood would increase the anion gap (acetate being the unmeasured anion) and lower serum bicarbonate. Common causes of elevated anion gap metabolic acidosis include diabetic ketoacidosis, lactic acidosis, poisonings, some inborn errors of metabolism, and renal failure.
Normal anion gap: Typically, normal anion gap acidosis will be accompanied by relative hyperchloremia, and thus is often called “hyperchloremic acidosis”. Common causes include excessive bicarbonate losses via the renal or GI system, or chloride administration during resolving anion-gap acidosis.
Some common causes of metabolic acidosis with elevated anion gap
Diabetic ketoacidosis (DKA): In this condition, runaway production of ketoacids plays the equivalent role of vinegar, inducing a metabolic acidosis. Typically beta-hydroxybutyrate is the major ketoacid but acetoacetate production is also excessive. Acetone levels are also elevated, but acetone is not an acid itself. Tissue perfusion can be compromised, inducing lactic acidosis as well, further exacerbating the metabolic acidosis. Laboratory findings include: (i) diminished serum bicarbonate, (ii) acidic pH, (iii) elevated anion gap, (iv) elevated serum beta-hydroxybutyrate and acetone. Insulin is used to halt ketoacid production. In severe DKA, the serum bicarbonate can approach zero and the pH can dip below 7.0. As ketoacidosis resolves, the bicarbonate climbs as does the pH while the anion gap normalizes. Often, the ketoacidosis resolves before the renal system can fully replace chloride with bicarbonate, leading to a transient hyperchloremic acidosis, though the pH is usually much improved by this stage.
Lactic acidosis: This can be caused by hypoxia, systemic inflammatory response syndrome, tissue injury, and more rarely specific inborn errors of metabolism.
Poisonings / intoxications: Causative agents include methanol, ethylene glycol, salicylates. Of note, many of these will cause an osmolar gap.
Uremia / severe end-stage renal failure: Due to retention of sulfate, phosphate and various organic acids.
Some common causes of metabolic acidosis with normal anion gap
GI loss of bicarbonate. Apart from the stomach, the GI tract is a bicarbonate secreting organ. Excessive loss of GI fluids, such as with diarrhea or pancreatic/biliary drains causes a metabolic acidosis with normal anion gap.
Renal loss of bicarbonate: In health, the kidney reabsorbs copious bicarbonate. Renal tubule dysfunction can interfere with this reabsorption and cause bicarbonate loss and metabolic acidosis with a normal anion gap.
Hyperchloremic acidosis during resolution of anion-gap acidosis. This is discussed above under DKA.
Mixed acid-base disorders
Acid-base disorders typically will induce a degree of compensation. Primary metabolic acid-base disturbances induce respiratory compensation, which occurs very rapidly. Primary respiratory acid-base disturbances induce metabolic compensation, though this occurs more slowly – over hours-to-days. Additionally, if the patient has more than one pathological condition at play, there may be additive respiratory plus metabolic disturbances. Ascertainment of these mixed acid-base disturbances requires a blood gas measurement. See footnote (f) for some free resources to learn more about these mixed disorders and their blood gas correlates. A simple summary follows, divided into two sections depending on whether the patient’s blood pH is acidic or alkaline.
Acidic pH
↓CO3– + ↓pCO2 = metabolic acidosis with respiratory compensation
Note: this is the most common scenario with metabolic acidosis.
↓CO3– + ↓pCO2 = respiratory alkalosis with metabolic compensation
Note: this is an occasion when a lower CO3– represents a physiological response. Illustratively, this scenario occurs at high altitudes. The thinner air at high elevations requires greater minute ventilation to maintain oxygenation. The increased ventilation induces a respiratory alkalosis, which then over time leads to compensatory decreases in serum bicarbonate mediated by renal losses. See PMID:27120676 .
These climbers are over 4,000 meters above sea level and thus expected to have a mixed acid-base disturbance including a physiological base deficit of roughly 4 mEq/L.
Footnotes
(a) Technically speaking, the reaction includes H2CO3 as an intermediate. In written form,: HCO3– + H+ ⇋ H2CO3 ⇋ H2O + CO2 . However, H2CO3 is unstable in aqueous systems and only exists very briefly and thus in effect does not play into the overall equilibrium.
(b) Conversely, respiratory acidosis occurs when blood carbon dioxide (pCO2) is too high.
(c) When H+ is added to bicarbonate, CO2 is produced. This appears as bubbles in the soda & vinegar experiment. In the body, much more minute quantities are involved and bubbles are not formed but rather the excess CO2 is dissolved in the blood and rapidly circulates to the lungs where it is exhaled.
(d) Likewise, if bicarbonate drops, there will be a shift of CO2 + H2O to produce H+ and CO3–, thus producing a net effect to raise H+ thus lowering the pH.
(e) This laboratory test is alternatively called “tCO2 or total CO2 (carbon dioxide)” or simply “serum CO2”. In fact, typically these tests measure the amount of bicarbonate plus carbon dioxide in the liquid sample. The molar amount of carbon dioxide in most clinical samples is far less than the amount of bicarbonate. Hence despite these alternative names, the reported value represents primarily serum bicarbonate. Factitiously low serum bicarbonate can occur. Importantly, phlebotomy-related issues can impact acid-base analytes. For example, samples smaller than intended for their collection tube can lose excess pCO2, thus altering the buffering equilibrium in favor of converting bicarbonate to carbon dioxide which is then lost from the sample. This is especially true in underfilled vacuum containers.
Post by Andrew Norris, MD PhD Director, Pediatric Endocrinology & Diabetes University of Iowa Stead Family Children’s Hospital
“it is incumbent upon the pilot/physician to keep ‘one hand on the throttle and one on the stick’ by providing both glucose and insulin when someone with type 1 diabetes is unable to eat…“
Managing type 1 diabetes is challenging, including for physicians. Often a physician naturally feels caught between two opposing fears.
Fear #1: “if too much glucose is given, the blood sugar might go too high”
Fear #2: “worse yet, if too much insulin is given then the blood sugar can go dangerously low”
These fears are real and represent real risks. The fear of these is especially heightened when managing diabetes in someone who is unable to eat. Unfortunately, these two fears present a false dichotomy that can lead to a cognitive error. The specific error logic is as follows:
Response to fear #1: “if glucose is not given, then the blood sugar can’t go high“
Response to fear #2: “if insulin is not given, then the blood sugar can’t go low“
The physician then writes orders that omit glucose (i.e. dextrose) from the IV fluids and under-dose insulin. Although this approach at first seems like a reasonable way to resolve the above conundrum, it can lead to serious issues. A useful analogy is that this is similar to flying a plane by cutting power to the engine and taking one’s hands off the stick. To better understand this, let’s first explore what happens when someone without diabetes is not given any glucose or carbs as they undergo fasting. The figure immediately below shows what happens to their plasma glucose, insulin and ketones levels.
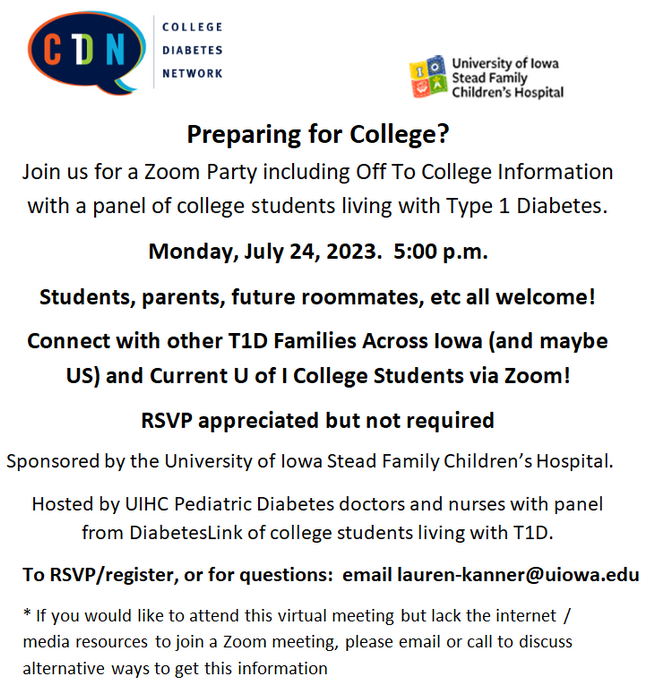
Normal Fasting Response: Plasma glucose (mmol/L), insulin (pmol/dL), and ketones (mmol/L) are shown in blue, green, and red respectively.
As shown in the figure, during fasting, glucose levels drop as expected, and in response insulin levels drop . But importantly, insulin levels do not drop to zero, but rather decline to a low but basal level. As insulin levels become low, this induces a catabolic state including the production of ketones. Key to this process is the fact that a low level of insulin remains to keep ketone production in check. To use our simplistic analogy, even though we let go of the airplane controls, autopilot has kicked in, courtesy of the beta-cells that maintain a basal degree of insulin secretion.
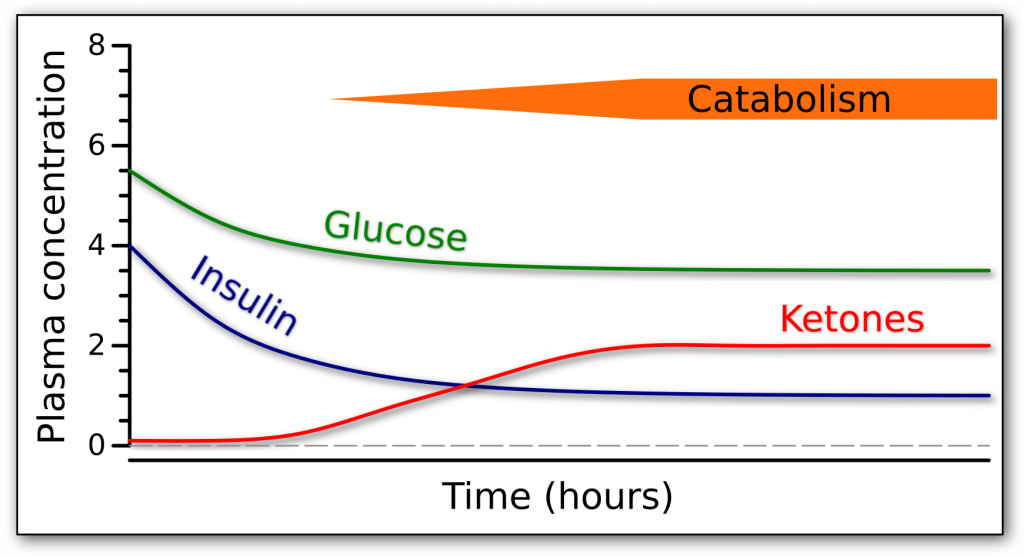
Let’s contrast this to what happens in someone with type 1 diabetes who can not make their own insulin. In this case, if insulin is not being given, levels eventually fall to zero, as shown in the next figure.
Fasting Response When Insulin Goes to Zero: Plasma glucose (mmol/L), insulin (pmol/dL), and ketones (mmol/L) are shown in blue, green, and red respectively. DKA stands for diabetic ketoacidosis, a life-threatening condition.
When insulin levels become abnormally low, two important things happen. Firstly, this triggers runaway gluconeogenesis, eventually leading to formation of new glucose and onset of spontaneous hyperglycemia. In other words, even though the person is not receiving glucose, their blood sugars rise because of the production of new glucose by their liver. Secondly, the abnormally low insulin levels allow runaway ketone production, eventually leading to diabetic ketoacidosis. To return to our simplistic analogy, our airplane has crashed and burned. When insulin levels reach zero, our engine can no longer burn fuel properly (i.e. insulin enables cells to properly utilize glucose), and gravity (i.e. run-away catabolism and ketone formation) ultimately wins.
Often, and typically in pediatrics, glucose is provided intravenously to patients without diabetes who can not otherwise obtain nutrition. It is informative to examine what happens to plasma insulin, glucose, and ketones in this situation, as shown in the next figure.
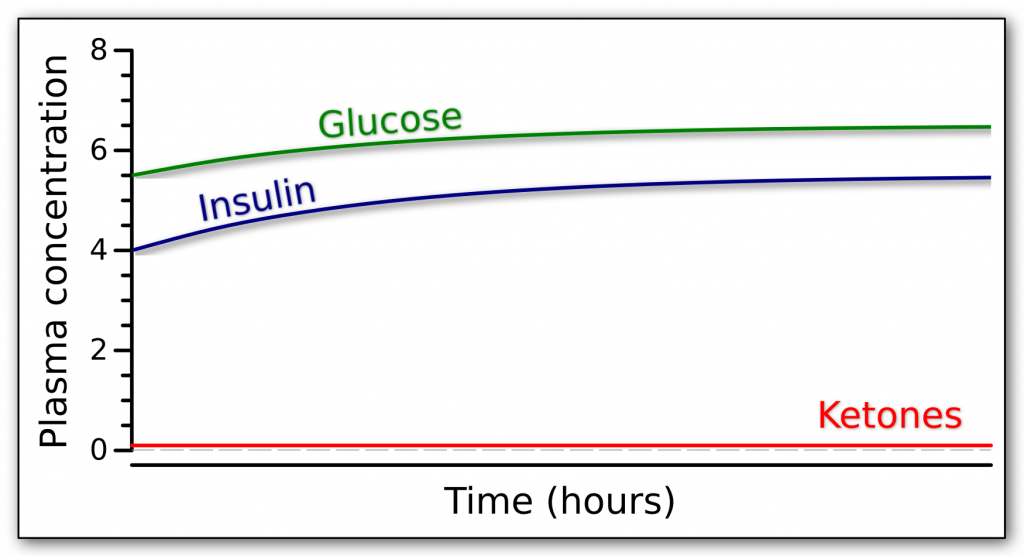
Response to Glucose Infusion in Persons without Diabetes: Plasma glucose (mmol/L), insulin (pmol/dL), and ketones (mmol/L) are shown in blue, green, and red respectively.
As is shown in the figure, the ongoing administration of intravenous glucose causes blood sugar to rise some, but the body responds by increasing insulin to compensate such that blood sugar remains normal. Importantly, because insulin does not reach low levels, ketone production remains suppressed and catabolism is avoided. This is a safe state for the patient. To keep a patient with diabetes safe, the physician can mimic this state by providing insulin and glucose. The insulin and glucose must be counterbalanced, and importantly insulin levels must be maintained always at a basal level, either through provision of long acting insulin or via intravenous insulin drip. Additionally , the blood sugars typically will vary. Despite this, because insulin is being continually supplied, ketone production is suppressed and the patient remains safe. The next figure illustrates this approach.
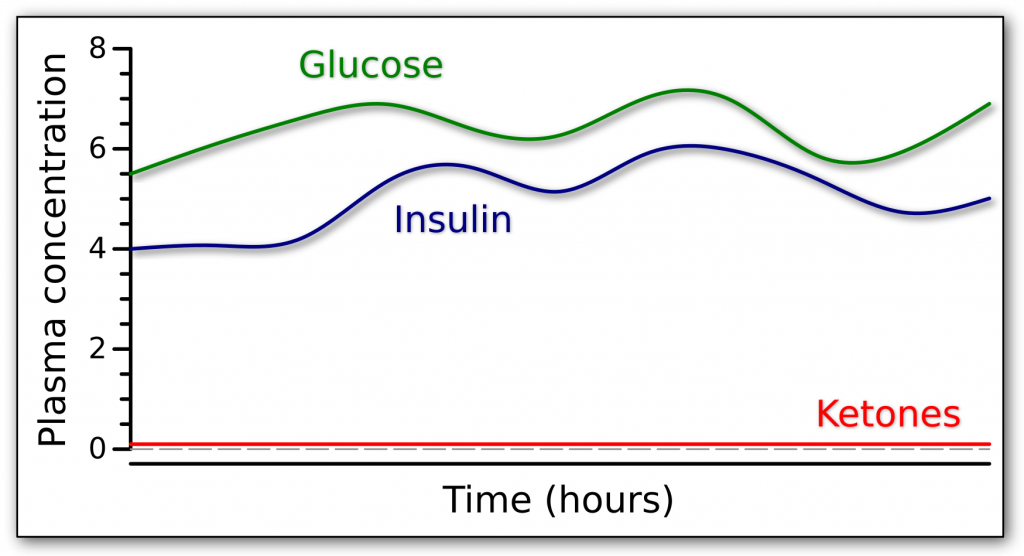
Provision of glucose and insulin in a fasting person with type 1 diabetes. Plasma glucose (mmol/L), insulin (pmol/dL), and ketones (mmol/L) are shown in blue, green, and red respectively.
Although the blood sugar varies, the patient remains safe because insulin levels do not fall to zero and because glucose is administered to maintain blood sugar levels. This way run-away catabolism and ketone formation are avoided, as are hypoglycemia and severe hyperglycemia.
Returning to our airplane analogy, functioning beta-cells are our usual autopilot. Someone with normally functioning beta-cells can be fasted or fed or given IV dextrose and remain euglycemic, avoiding hypoglycemia and ketoacidosis. In type 1 diabetes this autopilot is absent and it is incumbent upon the pilot to keep one hand on the throttle and one on the stick. Just like flying a plane, with study, practice and experience, the flight can be less turbulent.
In infants, children and adolescents with type 1 diabetes, the risks are heightened. Infants and children develop ketones at a more rapid pace than adults, and adolescence induces a state of physiological insulin resistance. Likewise, during illness and medical stress, the drive towards catabolism is increased, and the risks of crashing greater. Please know that your local pediatric endocrinology team remains happy to assist, helping ensure many safe landings.
Some notes: (1) Although the above discussion is simplified in many ways and the actual involved physiology is complex, nonetheless almost without exception out-of-control ketogenesis ensues when insulin levels become extremely low. (2) In the airplane analogy, gravity represents the incessant pull towards catabolism when insulin levels are low. (3) Although we think of dextrose containing fluids as driving major hyperglycemia, it should be remembered that 100 mL of D5 contains only 5 grams of glucose, about the same as 3 skittles or 2 saltine crackers. Interestingly, hepatic glucose production during routine fasting (i.e. overnight) is roughly the same as D10 containing IV fluids running at maintenance rates. For this reason, many metabolism experts advocate D10 containing IV fluids at maintenance rates to best avoid catabolism in patients both with and without diabetes. (4) Please know that blood glucose and plasma glucose are nearly equivalent, especially conceptually for the above purpose, and are thus used interchangeably above. (5) I don’t have actual data that this is the most common severe conceptual error in managing inpatient diabetes, but rather this reflects over a decades experience. (6) On a brief personal note, I would like to thank my life partner for proofing this.
“When these tumors occur in children, the manifestations are often different than in adults.“
Post by Andrew Norris, MD PhD Director, Pediatric Endocrinology & Diabetes University of Iowa Stead Family Children’s Hospital
A concise review of hormone-secreting pituitary tumors and their clinical syndromes appears in today’s New England Journal of Medicine. The article starts by noting that hormone secreting pituitary adenomas account for ~15% of all intercranial tumors. Although the article is informative and well written, it largely omits the characteristics of these disorders in childhood. When these tumors occur in children, the manifestations are often different than in adults. Below I have tabulated the anterior pituitary hormones that can be oversecreted by pituitary adenomas, and their common related childhood syndromes / symptoms. The table is listed in order of prevalence, from occasional to exceedingly rare (just a few case reports ever). Some of the symptoms of these conditions are common and non-specific (e.g. headache) and usually do not indicate a pituitary adenoma. Other symptoms almost always warrant an endocrine workup, especially growth failure, galactorrhea, precocious puberty, pubertal failure, gigantism, and acromegaly. On the flip side of hormone-secreting adenomas are pituitary adenomas that do not secrete hormones. Even though such adenomas do not secrete hormones, they eventually can lead to symptoms once their size impinges on local function. These manifestations can include visual field defects, headache, deficiency of pituitary hormones though prolactin can be modestly elevated due to pituitary stalk compression. Importantly, hormone secreting adenomas can also lead to these size-related effects as well.
Post by Andrew Norris, MD PhD Director, Pediatric Endocrinology & Diabetes University of Iowa Stead Family Children’s Hospital
In pediatrics and medicine we are taught various rules that help us interrogate a person’s health . However, there are a variety of endocrine disorders that alter normal physiology such that the usual rules no longer apply. Failure to recognize this can lead to erroneous interpretation of a person’s condition, sometimes with even fatal results
“Good urine output indicates that a child is well hydrated”
This is a stalwart rule in pediatrics. When a child is making plenty of urine, this proves that the child is well hydrated. In general this is sage advice, but there are important endocrine exceptions:.
Hyperglycemia / diabetes mellitus: When a child’s blood sugar is elevated, this produces an obligate osmotic diuresis. As a result, urine output remains brisk even when the child has become significantly dehydrated. To further exacerbate this, hyperglycemia leads to an osmotic fluid shift from the interstitium to the intravascular compartment, further increasing renal fluid output at the expense of worsening whole body hydration status. For these reasons, the child presenting with severe hyperglycemia is typically more dehydrated than the history and physical examination would suggest. There are cases where clinicians have been falsely reassured by a vomiting child’s brisk urine output, concluding that everything is fine when the child truly has severe hyperglycemia, with sometimes fatal consequences. Pediatricians in training are advised to become practiced and adept at asking children and families about any changes in thirst and urination, as this can be a fairly effective screening tool to assess for out-of-control undiagnosed severe diabetes.
Diabetes insipidus: In the child who has diabetes insipidus, urine output is not a reliable indicator of hydration status. When diabetes insipidus is not treated, brisk urine output occurs even in the face of dehydration. When diabetes insipidus is treated with vasopressin or DDAVP, urine output diminishes when the medication is active, even when hydration status is excellent.
“Children and adolescents can tolerate the physical stress of fever or vomiting.”
Typically, children can tolerate common physiological stressors such as significant febrile illness or vomiting / fasting during gastroenteritis. However, often children with underlying medical conditions do not tolerate such physiological stressors as well. Included in such underlying illnesses are several important and relatively common endocrine conditions
Adrenal insufficiency: An important component of the response to physiologic stress is increased secretion of adrenal hormones, especially cortisol. Children who are unable to secrete adequate amounts of cortisol can experience hypoglycemia, hyponatremia, and sometimes even cardiovascular collapse in response to physiologic stressors that ordinarily a child could tolerate without difficulty. Conditions in which cortisol secretion in response to stress can be impaired include panhypopituitarism, central adrenal insufficiency, congenital adrenal hyperplasia, Addison’s disease, iatrogenic adrenal suppression, and any form of hypoadrenalism. Children who have impaired mineralocorticoid secretion are at even greater risk for electrolyte imbalance, specifically hyponatremia and hyperkalemia, and cardiovascular collapse. common causes of mineralocorticoid deficiency include congenital adrenal hyperplasia and Addison’s disease. Fortunately stress dose hydrocortisone is an effective means to treat children with these conditions and enable them to better tolerate physiologic stressors.
Diabetes mellitus: Pediatric patients with diabetes require special attention to blood glucose and Insulin management during times of physiological stress. During such times, especially in patients with type 1 diabetes, there will be an increased risk of dysglycemia, ketones, dehydration, and diabetic ketoacidosis.
Hyperthyroidism: Patients who have active hyperthyroidism can experience significant deterioration during physiological stress and illness. In some cases, illness can precipitate thyroid storm, which can include life-threatening hyperthermia, confusion, diarrhea, tachycardia, arrhythmia, cardiovascular collapse, and coma.
“Children and adolescents tolerate exercise well”
In general children and adolescents can exercise seemingly ad infinitum. however there are a number of medical exceptions to this, including situations in which it is not entirely safe for a child to exercise vigorously. Several endocrine conditions are included among these exceptions to this common rule.
Hyperthyroidism: Children and adolescents with active hyperthyroidism typically experience a degree of exercise intolerance. If the hyperthyroidism is significant, some patients will even experience cardiovascular decompensation and/or hyperthermia triggered by vigorous exercise.
Ketonemia: children with diabetes can benefit greatly from exercise. however, when diabetes and ketones are present, exercise can exacerbate the degree of ketonemia, and in extreme cases can contribute to the development of diabetic ketoacidosis. standard advice during ketonemia in pediatric patients with diabetes is to administer supplemental insulin, optimize hydration, and delay a vigorous exercise until after the ketones have been cleared.
“Children do not experience electrolyte problems as long as renal function is normal and fluid / electrolyte intake is adequate.”
Although adequate fluid and electrolyte intake coupled with normal renal function is typically sufficient to maintain normal electrolyte balance, there are important exceptions to this rule especially in the endocrine system.
Diabetes insipidus: Patients with untreated diabetes insipidus generally develop hypernatremia during normal intakes of fluid and electrolytes. provision of greater than normal amounts of free water and or medical treatment of the diabetes insipidus is required to prevent hypernatremia.
SIADH (syndrome of inappropriate ADH secretion): Patients with SIADH have a tendency towards hyponatremia when provided normal amounts of fluid and electrolyte. Fluid restriction is commonly used to prevent hyponatremia in such patients.
Mineralocorticoid deficiency: Patients with untreated mineralocorticoid deficiency are prone to hyponatremia and hyperkalemia despite normal fluid and electrolyte intake. Common pediatric causes of mineralocorticoid deficiency include congenital adrenal hyperplasia and Addison’s disease.
“Failure of an infant to gain weight is a feeding issue.”
Many times, when an infant is not adequately gaining weight this can indicate various feeding issues. However, there are many medical diseases which can cause poor weight gain during infancy for reasons other than poor nutritional intake. There are several important to endocrine diseases among these conditions. Congenital adrenal hyperplasia typically causes poor weight gain and failure to thrive beginning towards the end of the first week of life. Neonatal Graves disease, when severe, presents with failure of a newborn to gain weight typically in the first week or two of life. Neonatal diabetes mellitus can present at various times in the first six months of life and can lead to poor weight gain.